




Coding Complications of Pregnancy: Hypertension, Pre-eclampsia, Eclampsia and ICD-10
Hypertension is dangerous during pregnancy because it may interfere with the placenta’s ability to deliver oxygen and nutrition to the fetus and has also been noted to be a contributing factor in low-birthweight babies. Pregnant patients may have other health problems too, such as gestational diabetes, that can contribute to the complexity of the pregnancy. These pregnancy complication may necessitate a patient be induced for delivery prior to the “normal” timeframe of 38-40 weeks of gestation. If induced for delivery, the patient will be closely monitored for a vaginal, or if more complications arrise, be delivered via cesarean section.
Women with hypertension in pregnancy have a higher risk of complications such as:
· Abruptio placentae. (Placental abruption)
· Cerebrovascular accident. (CVA)
· Disseminated intravascular coagulation. (DIC)
The fetus has an increased risk of:
· Intrauterine growth restriction. (IUGR)
· Prematurity.
· Intrauterine death.
As you can see in the table below, ICD-10cm gives us these codes to be used when hypertension is a factor in pregnancy, childbirth and the puerperium.
O10 Pre-existing hypertension complicating pregnancy, childbirth and the puerperium
O11 Pre-existing hypertension with pre-eclampsia
O12 Gestational [pregnancy-induced] edema and proteinuria without hypertension
O13 Gestational [pregnancy-induced] hypertension without significant proteinuria
O14 Pre-eclampsia
O15 Eclampsia
O16 Unspecified maternal hypertension
As we can see, not only do coders have to choose the correct code, the providers need to give good clear documentation for the coders to choose from. However, before we can correctly choose these codes, we need to have a good working knowledge of what the definitions are of the pregnancy hypertensive code-set. Unfortunately , the cause of pre-eclampsia is still unknown.
Pre-existing hypertension is defined as:
· a systolic blood pressure (BP) of 140 mm Hg or greater,
· and/or a diastolic BP of 90 mm Hg or more,
· either pre-pregnancy or before 20 weeks
Gestational hypertension (aka pregnancy-induced hypertension)
· Is the development of a new hypertension diagnosis in a pregnant woman after 20 weeks gestation without the presence of protein in the urine or other signs of preeclampsia.
· Can be considered severe when systolic blood pressure is ≥160 mmHg and/or diastolic blood pressure is ≥110 mmHg on two consecutive blood pressure measurements at least four hours apart
Preeclampsia is defined as:
· A condition in pregnancy characterized by abrupt hypertension (a sharp rise in blood pressure),
· Albuminuria (leakage of large amounts of the protein albumin into the urine)
· Edema (swelling) of the hands, feet, and face
· A headache that will not go away
· Seeing spots or changes in eyesight
· Pain in the upper abdomen or shoulder
· Nausea and vomiting (in the second half of pregnancy)
· Sudden weight gain
· Difficulty breathing
· Severe hypertension and signs/symptoms of end-organ injury are considered within the severe spectrum of the pre-eclampsia disease process.
o Note: In 2013, the American College of Obstetricians and Gynecologists (ACOG) removed proteinuria as an essential criterion for diagnosis of preeclampsia with severe features.
Eclampsia is defined as:
· The development of grand mal seizures in a pregnant patient with diagnosed pre-eclampsia, (in the absence of other neurologic conditions that could account for the seizure activity)
HELLP syndrome (Hemolysis, Elevated Liver enzymes, Low Platelets) is commonly defined as :
· a severe form of pre-eclampsia, OR
· HELLP syndrome can be considered an independent disorder from pre-eclampsia based upon the providers documentation)
Preeclampsia affects 3% to 5% of all pregnancies and any pregnant woman can get preeclampsia, but studies have shown that a patient is at a higher risk of pre-eclampsia if the provider has noted any of these risk factors:
· This is the first pregnancy
· A family history where the patient’s mother or sister had preeclampsia or eclampsia during pregnancy
· Patient is pregnant with a multiple gestation (eg: twins, triplets)
· Patient is under age 20 or over age 40 at the time of pregnancy
· The patient has a pre-existing diagnosis of high blood pressure, kidney disease, or diabetes
· The patient has a pre-pregnancy body mass index (BMI) greater than 30 (potential obesity)
· The patient was diagnosed with preeclampsia in a previous pregnancy
What to look for clinically – to choose the correct codes in ICD-10
Now that we are fully entrenched in ICD-10 coders will need to look for the above and verify that the provider has clearly stated the diagnosis when coding for a pregnant patient with symptoms of hypertension and/or pre-eclampsia. If only the symptoms are noted, it is warranted to then query the physician and ask if the symptoms correlate to a specific diagnosis, or are simply “separately identifiable” signs and symptoms.
Clinical Emergency Department Note:
HPI: 41-year female, G2P0A1, at 36 and 3/7 weeks, presents to the Emergency room with sever headache and confusion. Husband and mother both report that the patient has had episodes of muddled thinking for last ten days or more. Pregnancy has been uneventful. While in the Emergency Department, the pt complains of bilateral pulsing headache with no visual disturbances. Headache is aggravated with any movement and has not responded to Tylenol. Pt has had nausea x 3 days, no vomiting, but has symptoms of oliguria. Pt states “Cannot remember when I last urinated”. ROS includes RUQ pain. Patient reports good fetal movement, denies contractions, vaginal bleeding, or pelvic cramping. Patient also denies dizziness, loss of coconsciousness, tremors, seizures, SOB, chest pain. Patient denies tobacco, alcohol, or drug use. Patient states she took Tylenol 2 hrs ago, but without relief of headache.
Physical Exam:
Vital Signs: BP 142/94, T 98.9°F, P 94, R 22. Ht: 5’ 0” Wt: 151 lb.
Well nourished, well-groomed, A&Ox3, mood distressed.
HEENT, Respiratory and Cardiac exams all normal.
Abdomen: Fundal height consistent with 36 weeks, single fetus, vertex and engaged; fetal weight ~ 2,200g, FHR 142 bpm. Fetus small for gestational age.
Musculoskeletal: Adequate muscle tone + full AROM x4. Deep tendon reflexes were 4+/4+ with sustained knee and ankle clonus.
Extremities: Generalized edema present, 3+ bilateral edema LE. No cyanosis.
Vaginal exam: Cervix fingertip dilated and 5% effaced. The vertex was presenting at 0 station. Membranes intact. Laboratory: U/A 3+ proteinuria +2 glucose
Assessment/Plan: Severe pre-eclampsia. Will obtain Fetal ultrasound with bio-physicial profile and fetal non-stress test to assess fetal status. Proceed with Direct admit to Labor and Delivery unit for induction of labor. Admission orders: called and faxed to L&D unit nurse. Will contact patient’s primary OB to meet the patient at L&D and assume care for induction of labor in a pre-eclamptic advanced maternal age patient.
*****************************************************************************************
Operative Note:
Indication: 41-year-old patient that has been admitted to Labor and Delivery unit for induction of labor due to Severe pre-eclampsia. Induction attempted with IV Pitocin, but patient failed to progress. Fetus is cephalic per bedside ultrasound, and we will proceed with low transverse c/s
Patient was prepared and draped in the usual manner. Incision was made as noted above and carried down through the subcutaneous tissue, muscular fascia and peritoneum. Once inside the abdominal cavity, a low cervical transverse incision was made in the lower uterine segment after creating a bladder flap by both blunt and sharp dissection. With creation of the bladder flap, a transverse incision was made and the infant was delivered as a vertex. The placenta was removed and appeared normal w/3 vessel cord, cord blood was obtained. The infant was handed off to the nurses in attendance. The uterus was then exteriorized and brought out through the abdominal incision. We then closed the uterine incision in the usual manner with #1 Chromic suture in a running continuous manner. The bladder flap was inspected for hemostasis and closed with #2-0 Chromic in a running continuous manner as well. Number 0 Vicryl was used to close the fascia in a running continuous manner. The subcutaneous tissue and peritoneum were closed with #2-0 Vicryl suture in a running continuous manner. The skin was closed as noted above. Foley catheter inserted. Clear urine was noted. The sponge count was correct times 2. There were no complications. Estimated blood loss was 600 cc. Delivery of live male infant weighting 5 pounds 1oz having Apgar’s of 7 at one minute and 9 at five minutes. The patient was then awakened and taken to the Recovery Room in good condition
CPT Procedure Coding considerations for the above include:
A) Coding and Billing for the Emergency Department visit (99281 – 99285)
B) Coding and Billing for the Cesarean and/or Global Delivery Care by OB (Depending on care delivered)
a. 59510 Routine obstetric care including antepartum care, cesarean delivery, and postpartum care (Global Service)
b. 59514 Cesarean delivery only;
c. 59515 Cesarean delivery only; including postpartum care
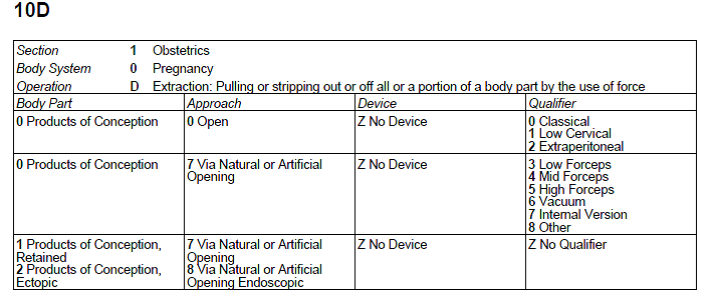
ICD10 pcs Procedure Coding Consideration
10D00Z1 Extraction, Products of Conception, Low Cervical cesarean section
ICD-10 cm Diagnosis Coding considerations include:
O14.13 Severe pre-eclampsia, third trimester
O61.0 Failed medical or unspecified induction of labor, delivered, with or without mention of antepartum condition
O09.513 Supervision of high-risk pregnancy with elderly primigravida third trimester N/A
Z3A.36 36 Weeks gestation
Z37.0 Single live birth
Coding Wrap up
In the clinical documentation by the provider, it was very well outlined and recorded to show the clinical diagnosis of severe pre-eclampsia. As per the ICD-10cm guidelines, In coding for obstetrics, if the trimesters are known, it is to be coded, in addition to the weeks of gestation.
When coding for this scenario in CPT, the E&M of the emergency room physician is considered “separately identifiable” from the obstetricians’ charges. Therefore, it is appropriate to code and bill for the emergency room physician, based upon the documentation.
When choosing the CPT code for the delivery, the coder will need to ascertain whether or not the delivery was performed as a “global” service. If the global service was performed by the OB provider, the entire spectrum of pregnancy care (which includes; antepartum, delivery care, and postpartum care services) should be billed. If the physician performed only the cesarean delivery and is not the global provider of service, then the cesarean only code should be billed. This also holds true if the provider performed the cesarean and is going to provide the postpartum care too.
ICD-10pcs – the coder needs to know whether or not the cesarean was performed as a classical, low cervical, or extraperitoneal cesarean section. In the operative note, the physician noted this was a low transverse cesarean section. The ICD-10 tables bring us to the code 10D00Z1 Extraction, Products of Conception, Low Cervical cesarean section.
If you are not seeing all the information you need in the clinical documentation to determine if the diagnosis is “hypertension” “pre-eclampsia” “Eclampsia” or “HELLP” syndrome, do not hesitate to query the provider and ask for additional clarification to be documented in the record.
Lori-Lynne A. Webb, CPC, CCS-P, CCP, CHDA, COBGC and ICD10 cm/pcs Ambassador/trainer is an E&M, and Procedure based Coding, Compliance, Data Charge entry and HIPAA Privacy specialist, with over 20 years of experience. Lori-Lynne’s coding specialty is OB/GYN office & Hospitalist Services, Maternal Fetal Medicine, OB/GYN Oncology, Urology, and general surgical coding. She can be reached via e-mail at webbservices.lori@gmail.com or you can also find current coding information on her blog site: http://lori-lynnescodingcoachblog.blogspot.com/.