





This is from my HCPro article published June 2016
In last weeks HCPro outpatient article we addressed tips for coding in the physician office, and the challenges with that side of medicine that affects both the physician and the physician office or group practice. In this article, we are addressing the inpatient side.
As discussed in the outpatient article, the disease of obesity is considered a major health problem In the US. Unfortunately, the disease process of obesity continues to be a major risk factor for the diagnoses in many other diseases such as diabetes, hypertension, sleep apnea, arthritis, and many, many more. Obesity is also medically associated with significant morbidity and mortality risk factors when any type of surgical or operative intervention(s), or even non-surgical hospitalization is necessary.
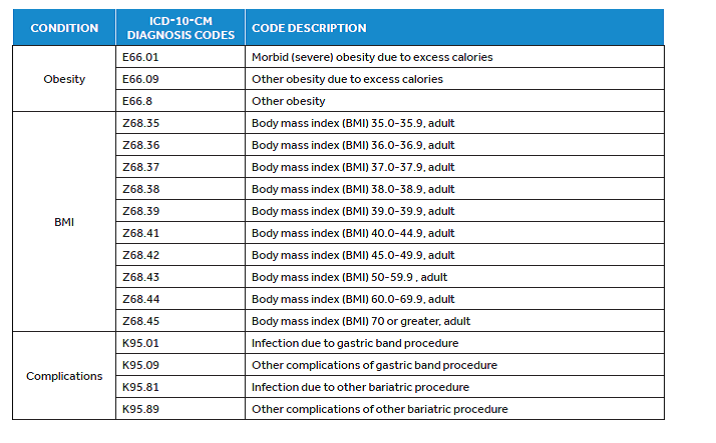
Most medical providers define and document obesity by the measurement of body mass index (BMI). The BMI is calculated by dividing a patient’s mass (kg) by his or her height (m2). A normal BMI is considered in the range of 18.5-24.9 kg/m2. A BMI of 25-29.9 kg/m2 is considered overweight. A BMI of 30 kg/m2 or greater is classified as obese; this classification is further subdivided into class I, II, or III obesity. In ICD-10cm, obesity and BMI are now easily identifiable, and should be documented in the patients’ records when obesity is being treated as a stand-alone diagnosis, or as part of a diagnosis with other disease processes that are impacted by obesity. The ICD-10 codes Z68.xx should be coded in addition to the diagnosis of obesity in the medical record and on your insurance claims
As we have been perfecting our ICD-10pcs coding skills with the ICD-10 tables; Let’s take a quick look again at the basics of code construction.
· All ICD-10-PCS codes have seven digits, each digit representing a specific character associated with procedures.
· Code assignment in ICD-10-PCS is a process of “constructing” the code by selecting values from the ICD-10 pcs code tables for each of the seven standard characters.
· The first three characters identify the code table that is used to complete the remaining four characters.
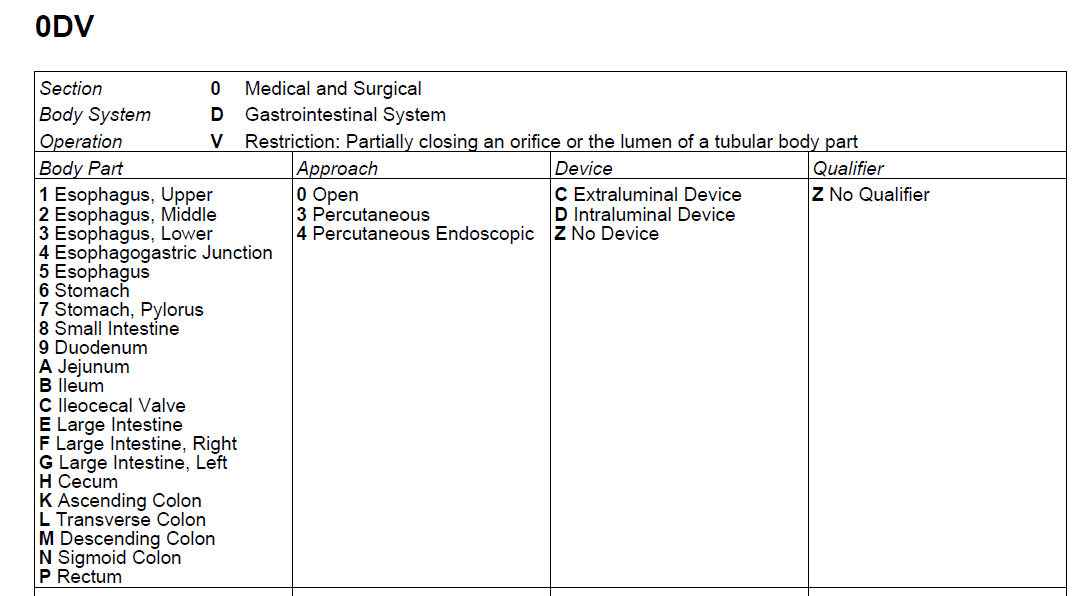
The basics of bariatric ICD-10-pcs code selection
· 1: Section: For bariatric procedures; the appropriate section is 0-Medical and Surgical.
· 2: Body System: Bariatric procedures involve the stomach and intestines, so code tables need to be referenced from; D-Gastrointestinal System.
· 3: Root Operation: When coding for the Root operation, in bariatric surgery, these are assigned according to the objective of the procedure. There are standard definitions to be reviewed in ICD-10 for root operations. When choosing the root operation, and the specific procedure that the physician is going to perform, there are three root operations that are most commonly used in bariatric coding.
1. Bypass: Altering the root of passage for the contents of a tubular body part, eg, Roux-en-Y gastric bypass
2. V-Restriction: Partially closing an orifice or the lumen of a tubular body part, eg, gastric banding
3. B-Excision: Cutting out or off, without replacement, a portion of a body part, eg, sleeve gastrectomy
§ Note: that because the procedure’s objective is the defining factor in assigning the root operation, some procedures that are not associated with bariatric coding may also use the same ICD-10-PCS code.
§ Note: The physician is not expected to document using ICD-10-PCS code descriptions. It is your responsibility as a coder to determine what the physician’s operative note documentation equates to in terms of ICD-10-PCS. AHIMA has stated that coder is not required to query the physician in these circumstances.
· 4: Body Part: In the respective ICD-10 pcs code tables the specific body part values that are available for you to choose from are for stomach, duodenum, and ileum.
· 5: Approach: The approach used for the bariatric surgical procedures performed are:
o Via laparotomy use 0-Open.
o Via laparoscopy use 4-Percutaneous Endoscopic.
· 6: Device: Interestingly in bariatric surgery, the device character is not used for surgical instruments that accomplish the procedure. The device character is used to describe the devices that remain in the patient’s body after the procedure is completed. (eg, implanted devices)
o For a Gastric banding procedures, the coder will use
§ C-Extraluminal Device because the band encircles the lumen of the stomach from the outside.
o If you are coding other bariatric procedures,
§ Z-No Device is most common choice when coding.
· 7: Qualifier: Qualifiers add further information to the ICD-10pcs code choice.
o For therapeutic procedures, the most common qualifier is Z-No Qualifier.
o For bypass procedures, the qualifier identifies the body part being bypassed to
§ eg… re-routing the digestive tract from the stomach directly to the ileum you would use the uses the qualifier B-Ileum.
Operative Report #1
Laparoscopic (Lap-Band) gastric band placement
The procedure consisted of laparoscopic placement of a gastric band (Lap-Band System), creating a proximal 15-mL pouch at the cardia.
The patient was positioned in an elevated recumbent position. The video monitor was located beyond the patient’s right shoulder. Pneumoperitoneum was created using a Palmer-Veress needle. The 10-mm optical trocar was inserted first, 10 cm below the xiphoid notch. Then, three 10-mm cannulas were placed under the rib margin. The fourth cannula on the left had a larger diameter (18 mm) to allow the introduction of the band. All cannulas were then shifted to the left when preoperative (re-review) ultrasound revealed an enlarged left liver lobe (>15 cm high) in the patient. A 10-mm liver retractor was inserted through a paraxiphoid cannula and the left lobe was elevated to expose the cardiac area and the diaphragmatic crus.
Gastric dissection started at the angle of the cardia by division of the phrenogastric ligament. We proceeded with the lap band procedure with a pars flaccida approach on the right side. Dissection on the left side was identical to that performed on the right. Over the lesser omentum, we opened the peritoneal sheet close to the edge of the right crus, then gradually created a retrogastric tunnel reaching the left crus and the phrenogastric ligament. Thus avoiding tthe use of a balloon. The band was secured by an anterior gastrogastric valve using four nonabsorbable seromuscular stitches. This covered the anterior part of the band completely. A methylene blue dye test was carried out with no leaks detected. The subcutaneous port components were then placed and verified as per our pre-operative marking. Patient was taken to PACU in good condition.
Coding Choices:
ICD-10pcs code: 0DV64CZ
Previous ICD-9 Vol 3: 44.95
CPT code: CPT Code: 43770 Laparoscopy, surgical, gastric restrictive procedure; placement of adjustable gastric band (gastric band and subcutaneous port components
Now as we look at some of the coding options for an “open” and “laparoscopic’ bypass procedure you will note the same table is used, but they are 2 completely different codes as one is an “open procedure” the other is “laparoscopic”
• Gastric bypass from stomach to ileum, performed via laparotomy
0D160ZB Bypass stomach to ileum, open approach
• Gastric bypass from stomach to jejunum, performed via laparoscopy
0D164ZA Bypass stomach to jejunum, percutaneous endoscopic approach

Diagnosis coding for bariatric medicine and bariatric surgery requires not only the definitions of the obesity, but notation of BMI. Most often the obesity diagnosis will remain as the primary reason for bariatric surgery, but any co-morbidities will also play into the DRG that will affect the reimbursement for the facility where the bariatric surgery is being performed.
According to AHIMA, they suggest including this into your medical records for the clinical documentation when referencing obesity and bariatric surgery:
• Obesity
– Morbid (severe)
° Due to excess calories
° With alveolar hypoventilation (Pickwickian syndrome)
– Drug Induced
° Document drug
– Other ° Due to excess calories, familial, endocrine
• Overweight
• Body Mass Index (BMI)
• Document any associated diagnoses/conditions
o Hypertension
o Type II Diabetes Mellitus
o Dyslipidemia
o Musculoskeletal, neurological or body size problems precluding or severely impairing quality of life (employment, family function or ambulation)
o Life-threatening Cardiopulmonary Problems (sleep apnea, obesity-hypoventilations syndrome or obesity-related cardiomyopathy)
o Coronary Artery Disease
o Obesity-Related Cardiomyopathy
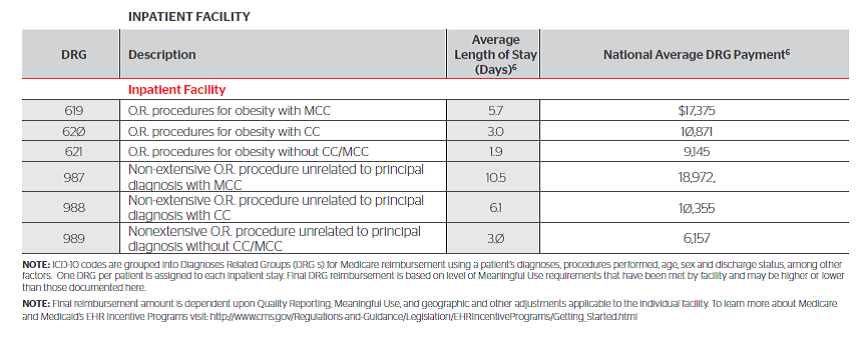
As we can see from this table below of 2016 “estimated” DRG’s and reimbursements for facilities, a bariatric surgery can be very lucrative for your facility. The DRG assignments will need to be carefully reviewed when coding out bariatric surgery to obtain the highest appropriate DRG’s.
Currently, there has been an increase in private insurance companies covering bariatric surgical procedures if the patient meets the standard criteria for morbid obesity. However, some carriers may not cover it at all, and it may be a self-pay only option for the patient. Medicare has been one of the primary payers that have approved bariatric surgery, with the resulting off-set of better health for the patient, and a reduced risk of long-term medical complications from the co-morbidities.
Medical necessity plays a huge part in a patient being able to undergo a bariatric surgery. If the patient is morbidly obese and has a body mass index (BMI) of 40 or higher an insurance carrier is more likely to approve or pre-authorize a surgery. Another criteria that may be imposed, is if the patient has been obese for the past five years or longer, and has
attempted, under a physician’s care; other methods of weight loss for at least two years. These may include behavior modification, psychological evaluations, in addition to specifically proven medically regulated diets such as “Optifast” “Medifast” or even drug therapies such as orlistat (Xenical), lorcaserin (Belviq), phentermine and topiramate (Qsymia), buproprion and naltrexone (Contrave), and liraglutide (Saxenda). If the patient has comorbidities such as hypertension, diabetes, sleep apnea, degenerative arthritis, and heart disease that increase the consideration of medical necessity for surgery.
In addition there are some patients in which they would not qualify for bariatric surgery. Absolute contraindications to bariatric surgery are active substance abuse and psychiatric personality disorders. In addition, previous abdominal surgeries or previous bariatric procedures that were ineffective are not necessarily contraindications, but the patient may not be approved for more extensive bariatric surgery. Some studies have borne out that procedures which alter the size of the stomach and restrict food intake, may exacerbate some eating disorder. If the patient has a history of a true anorexia nervosa, they are generally considered not eligible for bariatric surgery.
As a coder, good documentation from your providers in the H&P help ensure you are able to clearly code and report the operative session(s), with the diagnosis of obesity and all additional diagnoses that are impacted by the obesity (medical necessity). All of these criteria go hand in hand with good quality patient care and correct coding and billing of claims. By working closely with your providers, you can ensure good clean claims, and reduce your overall risk of audit inquiry and financial recoupment of paid claim services.
Lori-Lynne A. Webb, CPC, CCS-P, CCP, CHDA, COBGC and ICD10 cm/pcs Ambassador/trainer is an E&M, and Procedure based Coding, Compliance, Data Charge entry and HIPAA Privacy specialist, with over 20 years of experience. Lori-Lynne’s coding specialty is OB/GYN office & Hospitalist Services, Maternal Fetal Medicine, OB/GYN Oncology, Urology, and general surgical coding. She can be reached via e-mail at webbservices.lori@gmail.com or you can also find current coding information on her blog site: http://lori-lynnescodingcoachblog.blogspot.com/.